Ultrasound guided peripheral and central venous access has become more common while simultaneously decreasing complications and increasing first pass success. Landmark guided palpation has historically been considered the standard of care when placing arterial lines, however the use of ultrasound is challenging that notion as anatomic landmarks are not helpful in 30% of patients.1 Additionally, increasing obesity and hemodynamic instability can make radial arterial line placement even more difficult when using landmark-guided palpation alone. The literature comparing the different methods of arterial line placement is limited to two prospective studies. The first assessed second- and third-year emergency medicine residents while the second study evaluated only four emergency medicine attendings, all with extensive ultrasound training and experience.2,3 The authors of this study sought to compare radial arterial line placement using ultrasound vs landmark guided palpation performed by novice emergency medicine interns with respect to overall success.
REBEL Cast Ep90 – US- vs Landmark-Guided Palpation for Radial Arterial Line Placement
Paper: Gibbons RC, et al. Ultrasound Guidance Versus Landmark-Guided Palpation for Radial Arterial Line Placement by Novice Emergency Medicine Interns: A Randomized Controlled Trial. J Emerg Med. 2020 Sep 8: PMID: 32917440
Clinical Question:
Does the use of ultrasound or landmark-guided palpation achieve a higher success of radial arterial line cannulation?
What They Did:
Single-center, prospective, randomized control trial at an urban academic level 1 trauma center
Prior to the start of the study, the investigators changed the primary outcome from the number of attempts to overall success
Randomized to one of the following two groups for arterial line placement:
Ultrasound guided (USG)
Landmark-guided palpation (LMGP)
A novice emergency medicine (EM) intern placed all arterial lines supervised by a second- or third-year EM resident who did not provide any tactile or physical assistance.
An independent research assistant blinded to the study’s objectives assessed the operator for the study outcomes listed below
If unable to cannulate the artery in the landmark-guided palpation technique after 3 attempts or 15 minutes, operators crossed over to ultrasound guided placement
No senior resident or faculty performed any of the cannulations including when a crossover method was necessary
Inclusion Criteria:
Adult English and Spanish-speaking emergency department patients ≥ 18 years old who required placement of an arterial line placement for hemodynamic monitoring and cardiopulmonary resuscitation based on attending physician discretion
Exclusion Criteria:
None mentioned
Outcomes:
Primary
Overall success of arterial line placement
Secondary
First-pass success
Number of attempts
Time to completion
Complications (i.e. hematoma, infection and arterial occlusion)
Results:
A total of 40 patients were enrolled, 20 in both groups
The ultrasound group had 11 different interns and the landmark group had 13 different interns (18 total interns in program means some residents performed both techniques)
Critical Results:
Of the 20-landmark guided arterial lines attempted, the 17 that were initially unsuccessful had crossed over to be successfully placed under ultrasound guidance
Of the failed LMGP, USG crossover was 100% successful with a mean of 1.37 attempts and 180s for placement
All 20 patients in the USG group had 100% overall success
Strengths:
Authors attempted to answer a clinically relevant question that is often frequently debated now that ultrasound is more prevalent in clinical practice
Tried to include all the possible complications, both immediate and delayed, that may result from arterial line placement
The authors were very clear in their definitions (i.e. Novice, supervising resident, time, complications, etc.)
The exact method used to place an arterial was standardized and explicitly written out by the authors
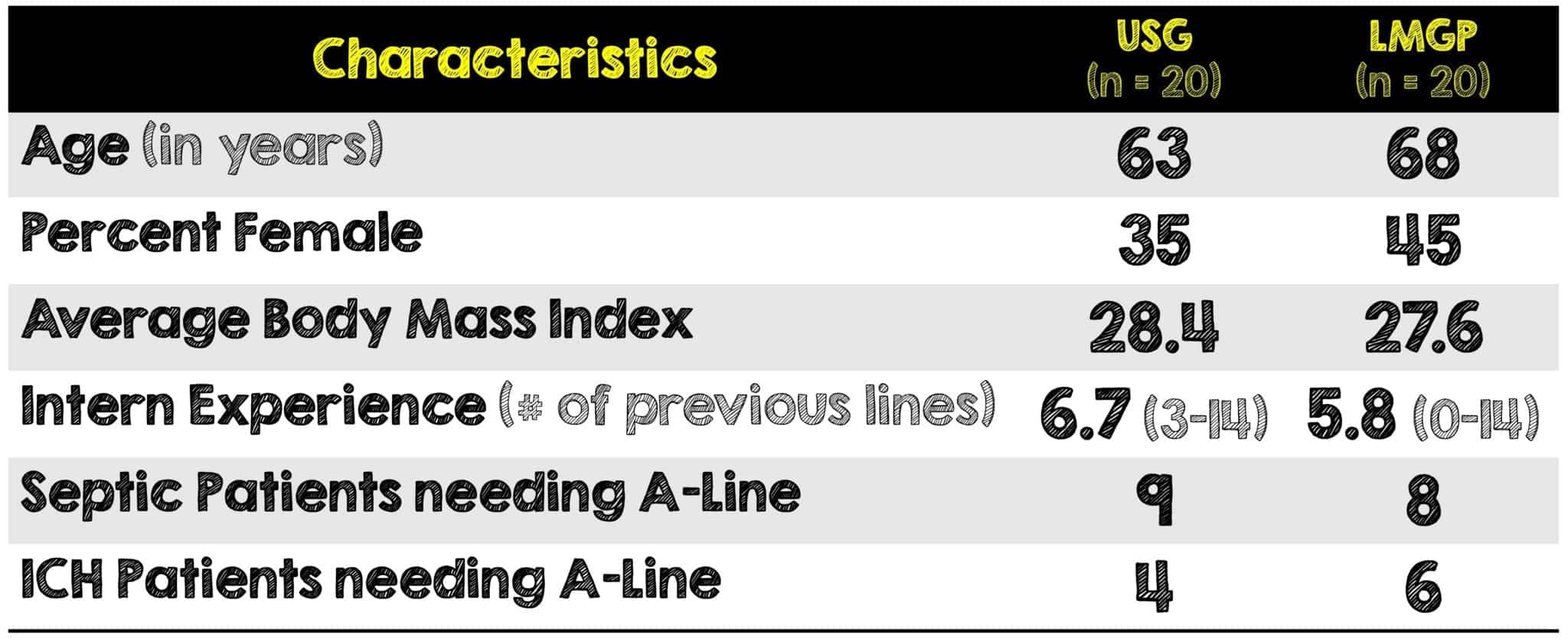
Patient characteristics, intern experience, and indications for arterial line placement were similar between groups
Limitations:
Single center urban academic center with a small sample size
Large ultrasound presence in the department and faculty may have unconsciously biased results to favor the USG group
Patient enrollment was a convenience sample, thus potentially introducing selection bias
Authors did not account for previous POCUS and procedural proficiency of the interns (i.e. when each participant completed the 4-week ultrasound rotation before or after participating in this study)
Authors did not account for any specific verbal guidance by supervising residents on needle/probe manipulation or ultrasound setting adjustments
As the authors mention, landmark guidance may have been more difficult and prone to failure in hypotensive patients given their subsequent vasoconstriction (i.e. Did not account for vasopressor use or blood pressure differences between patients prior to cannulation). In fact, the only mention as to how hemodynamically unstable (if at all) some of these patients were, was the indications of possibly needing arterial line placement.
Discussion:
This is the first randomized control trial looking at arterial line placement using ultrasound by EM interns
Study results, specifically LMGP match a prior study comparing placement by second- and third-year residents as well as another study comparing placement by four attendings
Authors were looking for a 40% difference in the primary outcome which was based on previous evidence
This emergency department and its subsequent residency program is very ultrasound friendly. They also have an ultrasound fellowship program thus creating a more receptive and positive culture towards the use of ultrasound for this procedure compared to other emergency departments that may not be as savvy in ultrasound
All EM interns participated in an introductory 4-hour ultrasound procedure course taught by EM ultrasound-faculty specifically reviewing central and arterial line placement using dynamic needle-tip guidance. Additionally, each intern is required to complete a 4-week emergency ultrasound rotation. Although, the mean number of previous arterial lines was 6, it’s unclear where the intern-operator was in their course of training (ie. having just come off orientation or their ultrasound rotation) prior to participating in this study
Important Definitions:
Novice was defined as having placed less than 15 arterial lines and the supervising residents each had previously placed more than 25 arterial lines. These numbers were arbitrarily defined by the authors using the rationale of trying to compare each technique without the bias of significant previous experience with either method
Time to completion was defined as time elapsed from needle insertion to complete cannulation of the catheter. Time to suture, time to apply a sterile dressing and time to connect to the monitor were not included
Defined alternative methods as changing direction or withdrawing the needle and having to puncture again
Vasospasm was not included in the predefined complications because the providers did not have a means to assess for this. Complications were recorded by the research assistant at the time of the procedure and then the authors went back to perform a chart abstraction within 7 days of line placement to record any delayed complications
Author’s Conclusions:
USG improved first-pass and overall success of radial arterial line cannulation while reducing time to access and attempts when used by novice emergency medicine interns
Our Conclusion:
In this study of novice emergency physicians, ultrasound-guided radial arterial line placement had a better first-pass and overall success, while minimizing attempts and complications compared to a landmark-guided palpation technique. This study shows that ultrasound guided arterial line placement is safe and more efficient approach to radial arterial cannulation. Although, the complication rates were low in this trial, complications have been associated with more frequent cannulation attempts and prolonged time to placement.
Clinical Bottom Line:
Ultrasound-guided arterial line placement improved first pass and overall success when compared to landmark guided placement of radial arterial lines in novice emergency physicians
REFERENCES:
Gibbons RC, et al. Ultrasound Guidance Versus Landmark-Guided Palpation for Radial Arterial Line Placement by Novice Emergency Medicine Interns: A Randomized Controlled Trial. J Emerg Med. 2020 Sep 8: PMID: 32917440
Wilson C, et al. Comparison of ultrasound-guided vs traditional arterial cannulation by emergency medicine residents. West J Emerg Med 2020; PMID: 32191193
Shiver S, Blaivas M, Lyon M. A prospective comparison of ultrasound-guided and blindly placed radial arterial catheters. Acad Emerg Med 2006; PMID: 17079789
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srreziae)