

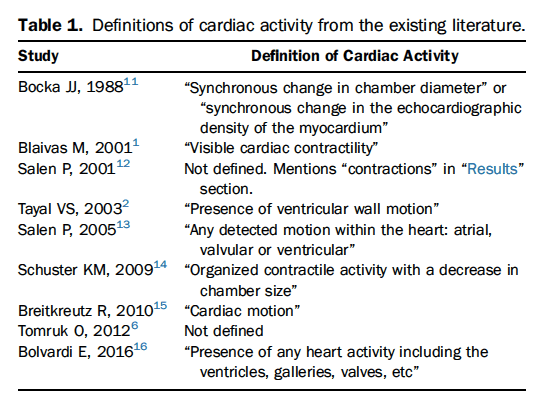
 Background: Point of Care Ultrasound (POCUS) has gained wider use in resuscitation of patients presenting with cardiac arrest. POCUS can play an important role in determining the etiology of arrest as well as being used to determine the presence or absence of mechanical activity. The REASON study demonstrated that patients with PEA or asystole without cardiac activity on POCUS are extremely unlikely to survive to hospital discharge though this study did not investigate the more important question of a survival with a good neurologic outcome. (Gaspari 2016). In light of this as well as other evidence, some have proposed that the absence of cardiac activity may be adequate to declare resuscitation futility and stop resuscitative efforts. However, there is a lack of agreement on what defines cardiac activity (see table 1). Due to this, and other factors, the level of agreement between physicians in interpretation of cardiac standstill is unknown.
Background: Point of Care Ultrasound (POCUS) has gained wider use in resuscitation of patients presenting with cardiac arrest. POCUS can play an important role in determining the etiology of arrest as well as being used to determine the presence or absence of mechanical activity. The REASON study demonstrated that patients with PEA or asystole without cardiac activity on POCUS are extremely unlikely to survive to hospital discharge though this study did not investigate the more important question of a survival with a good neurologic outcome. (Gaspari 2016). In light of this as well as other evidence, some have proposed that the absence of cardiac activity may be adequate to declare resuscitation futility and stop resuscitative efforts. However, there is a lack of agreement on what defines cardiac activity (see table 1). Due to this, and other factors, the level of agreement between physicians in interpretation of cardiac standstill is unknown.
Clinical Question: How much variability exists in the interpretation of cardiac standstill on POCUS amongst physicians?
Article: Hu K et al. Variability in Interpretation of Cardiac Standstill Among Physician Sonographers. Ann Emerg Med 2017. PMID: 28870394
Population: Survey respondents were residents, fellows and faculty attending ED-ICU combined ultrasound rounds at a combined conference (three academic institutions).
Outcomes:
- Primary: Variability in interpretation of cardiac standstill among respondents
- Secondary: Variability among subgroups based on specialty, training level and self-described POCUS experience
Design: Cross-Sectional convenience sample survey. Participants were shown 15, 6-second deidentified ultrasound clips of patients with pulseless arrest and given up to 20 seconds to answer whether the clip demonstrated cardiac standstill or not.
Excluded: Physicians that did not register demographic information (specialty, training level etc).
Definitions of Cardiac Activity:
Definitions:
Krippendorff’s alpha = assessment of interrater reliability among physicians, similar to Fleiss’s kappa but thought to be more reliable in situations with missing data points
- Range of 0 to 1:
- 0 = poor agreement
- Customary to require alpha ≥0.80 for agreement, but tentative conclusions can be drawn at alpha ≥0.667
- 1 = perfect agreement
Primary Results:
- Physician sonographers included: 127
- Emergency Medicine: 94 (74%)
- Critical Care: 15 (12%)
- Cardiology: 4 (3%)
- Training Level
- Resident: 80 (63%)
- Fellow: 11 (9%)
- Attending: 24 (19%)
- POCUS Skill Level
- Basic: 68 (54%)
- Advanced: 37 (29%)
- Expert: 7 (6%)
Critical Findings:
- Interrater Agreement (Primary Outcome)
- Overall: moderate agreement (alpha = 0.47)
- Variable agreement across US clips
- Interrater Agreement by Subgroup
- Moderate agreement seen across specialty, training level and US experience
- Fair agreement among critical care physicians
Strengths:
- Study asks an important diagnostic question that has not been previously addressed
- Majority of respondents self-reported “basic skill level” which may make study more generalizable (in comparison to just having expert level operators)
Limitations:
- Non-random, convenience sample of participants
- Majority of respondents self-reported “basic skill level” which may skew analysis towards disagreement
Authors Conclusions: “According to the results of our study, there appears to be considerable variability in interpretation of cardiac standstill among physician sonographers. Consensus definitions of cardiac activity and standstill would improve the quality of cardiac arrest ultrasonographic research and standardize the use of this technology at the bedside.”
Our Conclusions: We agree with the authors that this study, though limited by it’s methodology and convenience sample, demonstrates significant disagreement between providers as to the interpretation of cardiac standstill on POCUS.
Potential to Impact Current Practice: This study cannot be used to impact clinical practice but should cause some pause for thought for providers who are currently using POCUS in cardiac arrest as part of their protocol for termination based on cardiac standstill.
Bottom Line: The use of POCUS to declare death and stop resuscitation is predicated on a clear ability to establish the presence of cardiac standstill. The low level of agreement of providers likely reflects the absence of a single definition of standstill as well as calls for increased training and assessment. A unified definition of standstill would be extremely helpful not only in future research but in cardiac arrest care as well.
For More on This Topic Checkout:
- Core EM: ED POCUS in OHCA – The REASON Study
References:
- Gaspari R et al. Emergency Department Point-Of-Care Ultrasound in Out-Of-Hospital and in-ED Cardiac Arrest. Resuscitation 2016; 109: 33 – 39. PMID: 27693280
Post Peer Reviewed By: Salim R. Rezaie (Twitter: @srrezaie)






