







REBEL Cast Ep114: High Flow O2, Suspected ACS, and Mortality?
Background: Historically, we have treated acute coronary syndrome with supplemental ...

REBEL Core Cast – Basics of EM – Chest Pain
Take Home Points Take chest pain seriously – ACS and PE ...

Retrospective Validation of High-Sensitivity Troponin with 5 Clinical Decision Instruments
Background: Chest pain is the second most common reason for presentation ...

GRACE Guidelines: A Pragmatic Approach to Recurrent Low-Risk Chest Pain
In the United States, a patient with chest pain presents ...

Chest Pain and Chemotherapy: 5-FU Induced Coronary Vasospasm
58 y/o female with colorectal cancer recently started on continuous ...

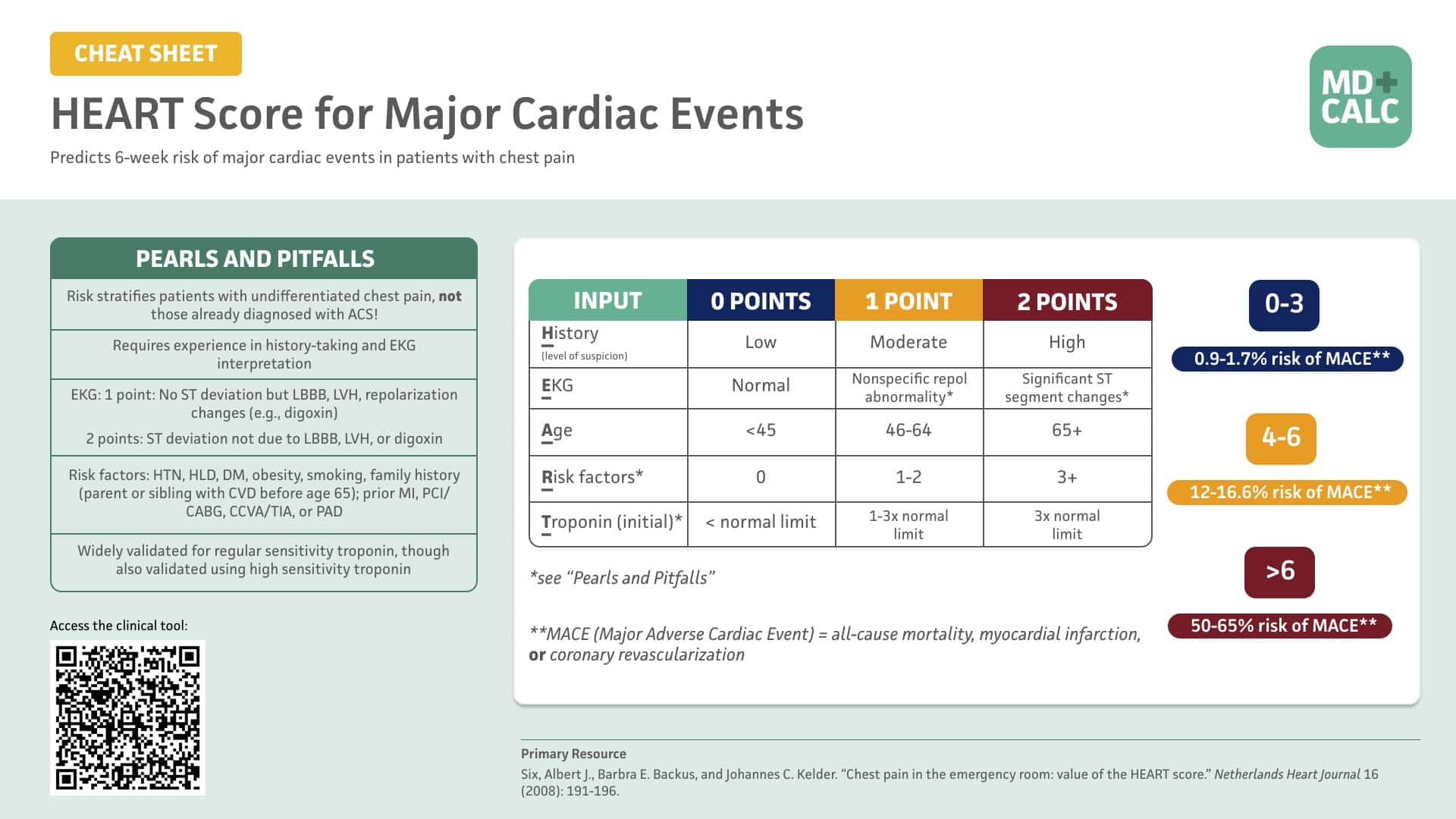
The HEAR Score: Does Very Low-Risk Acute Chest Pain Not Require Troponin Testing?
Background: Chest pain is one of the most frequent presenting ...
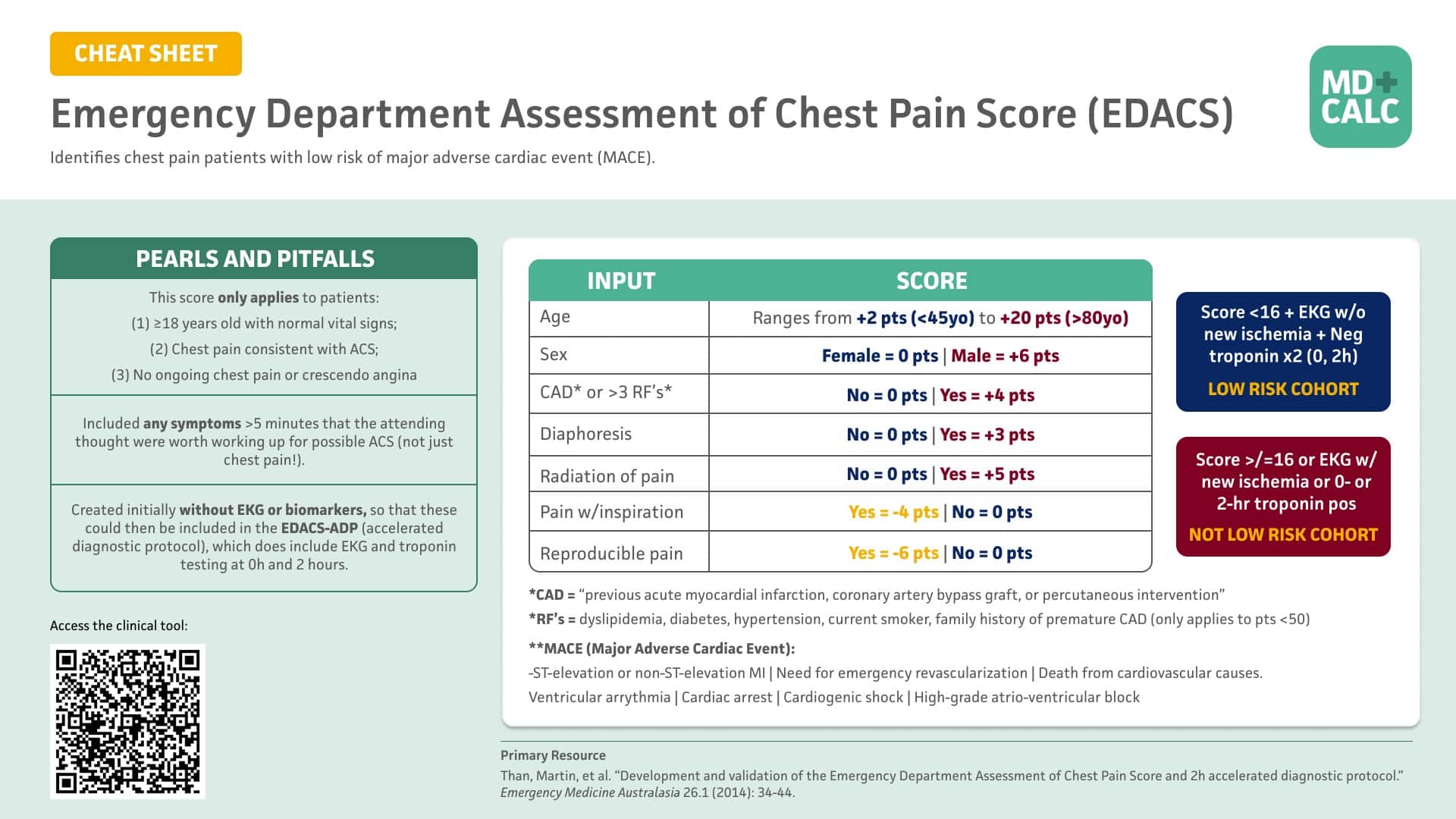
Cite this article as: Eric Steinberg DO, MEHP, "MDCalc Wars: HEART Score Vs. EDACS", REBEL EM blog, June 30, 2025. Available at: https://rebelem.com/mdcalc-wars-heart-score-vs-edacs/.










{kind=link}
{kind=link}