

Background: The clinical burden of severe COVID-19 triggered a pharmaceutical race to find effective, easily accessible, oral treatments that could decrease the morbidity and mortality associated with the disease. Nirmatrelvir is an oral antiviral agent that inhibits the SARS-CoV2 main protease involved in viral replication. It is administered with ritonavir, which inhibits the cytochrome P450-3A4 pathway, increasing the bioavailability and effectiveness of Nirmatrelvir. In December 2021, there was an emergency use authorization issued by the Food and Drug Administration (FDA) for the use of nirmatrelvir-ritonavir (Paxlovid) in high-risk patients with COVID-19.
The emergency use authorization was largely based on the study, an industry-run trial that looked at treatment for mild-to-moderate COVID-19 in patients at risk of progression to severe disease.1 The EPIC-HR study touted significant relative risk reduction for nirmatrelvir-ritonavir when looking at hospitalization from COVID-19 and death from any cause when compared to placebo.1 Subsequent have yielded varied and inconsistent results on the efficacy of nirmatrelvir-ritonavir with the Cochrane review concluding that there is “low-certainty” to “very low-certainty” evidence for nirmatrelvir-ritonavir in COVID-19 outpatients infected with the Delta or the Omicron variant of SARS-CoV2.2
The current phase 2-3 EPIC-SR trial examines the efficacy and safety of nirmatrelvir-ritonavir among standard-risk patients (without risk factors for severe COVID-19, either unvaccinated or without vaccination within the last year) as well as fully vaccinated patients at high-risk for progression to severe COVID-19.
Paper: Hammond J, et al. Nirmatrelvir for Vaccinated or Unvaccinated Adult Outpatients with COVID-19. N Engl J Med. 2024. PMID 38598573
Clinical Question: In non-hospitalized adults with mild to moderate COVID-19 at standard risk of developing severe disease, does the use of nirmatrelvir-ritonavir compared to placebo reduce the time to sustained alleviation of COVID-19 symptoms?
What They Did:
- Phase 2-3, double-blind, 2-arm, randomized placebo-controlled trial from August 2021 to July 2022
- Randomization was stratified by geographic region, vaccination status, and COVID-19 symptom onset.
- Enrolled adult outpatients with COVID-19
- Unvaccinated or not vaccinated within the last year without risk factors for severe disease
- Fully vaccinated adult outpatients with at least 1 risk factor for severe disease.
- Eligible nonhospitalized symptomatic patients with confirmed COVID-19 were randomized 1:1 to receive either:
- Nirmatrelvir-Ritonavir Q12h for 5 days (10 doses total)
- Placebo with inactive filler ingredients Q12h for 5 days (10 doses total)
- Participants used an electronic diary to document medication administration as well as presence and severity of COVID-19 signs or symptoms on 4-point scale (0, absent; 1, mild; 2, moderate; 3, severe)
- Total study duration was 24 weeks, with study intervention through Day 5 or 6, efficacy assessments through Day 28, safety follow-up through Day 34, and long-term follow-up at Weeks 12 and 24.
Population:
Inclusion Criteria:
- Adults > 18 years of age
- Confirmed SARS-CoV-2 infection as determined by RT-PCR or rapid-antigen testing
- Onset of signs and symptoms of COVID-19 within 5 days before the day of randomization
- At least 1 of the prespecified signs or symptoms was attributed to COVID-19 on the day of randomization
Exclusion Criteria:
- At least 1 characteristic or underlying medical condition associated with an increased risk of developing severe illness from COVID-19
- Age ≥ 65
- BMI ≥ 30 kg/m2
- Current smoker (last 30 days) and history of at least 100 lifetime cigarettes
- Chronic lung disease, cardiovascular disease, cerebrovascular disease, HTN, DM, chronic kidney disease or dialysis dependent, active liver disease, sickle cell disease
- Neurodevelopmental disorders
- Active malignancy (other than localized skin cancer)
- Medical-related technological dependance (ex CPAP)
- Immunosuppressive disease (HIV, immune deficiencies, bone marrow or organ transplant recipients) or prolonged use of immune-weaking medications
- Previous confirmed COVID-19 infection
- History of hospitalization for medical treatment of COVID-19
- Received or is expected to receive monoclonal antibody treatment, other antiviral treatment, or convalescent COVID-19 plasma
- Suspected or confirmed concurrent systemic infection other than COVID-19
- Current hospitalization or anticipated need for hospitalization within 48 hours after randomization
- Comorbidities or laboratory abnormalities requiring hospitalization and/or surgery short-term
- Suicidal ideation/behavior
- Use of medications or substances dependent on CYP3A4 pathway
- Recipient of any SARS-CoV-2 vaccination within 12 months of screening
- New abnormalities in liver function testing, GFR, ANC within past 6 months of screening visit
- SPO2 < 92% on room air at rest within 24 hours prior to randomization
- Females who are pregnant or breastfeeding
Interventions:
- Nirmatrelvir-ritonarvir every 12 hours for 5 days
Control:
- Placebo with inactive filler ingredients every 12 hours for 5 days
Outcomes:
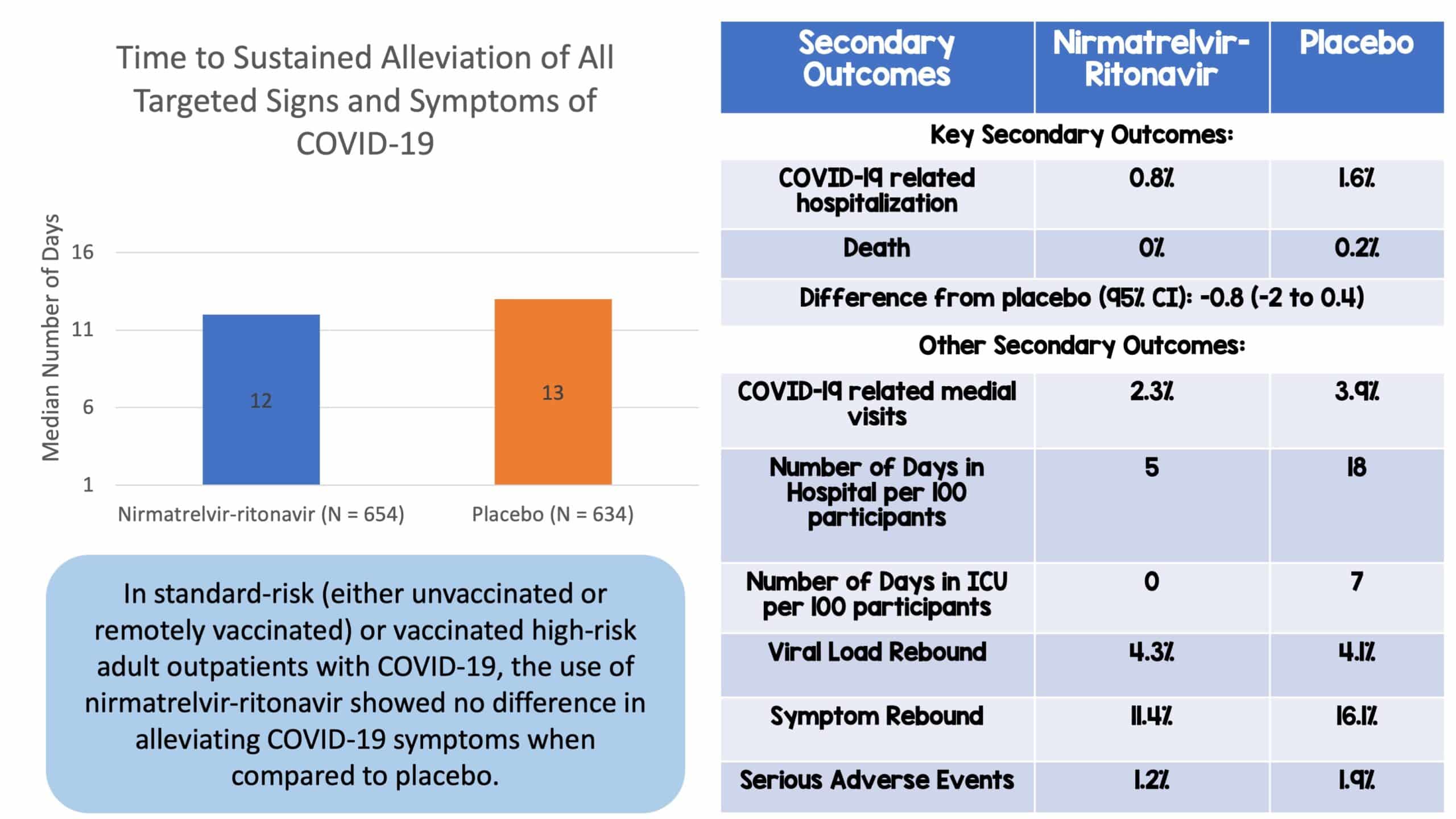
- Primary Outcome: Time (days) to sustained alleviation of all targeted COVID-19 signs/symptoms through Day 28.
- Targeted Symptoms: “Cough, shortness of breath or difficulty breathing, feeling feverish, chills or shivering, muscle or body aches, diarrhea, nausea, vomiting, headache, sore throat, and stuffy or runny nose.”
- Sustained Alleviation: Considered to have occurred on first of 4 consecutive days during which all symptoms that had been scored as moderate or severe and as mild or absent at baseline were scored as mild or absent and as absent, respectively.
- Key Secondary Outcome: COVID-19 related hospitalization or death from any cause through day 28.
- Other Secondary Outcomes:
- Number of COVID-19 related medical visits through day 28
- Number of days in hospital and ICU stay in participants with COVID-19 related hospitalization through day 28
- Viral load
- Viral load rebound
- Symptom rebound
- Adverse events leading to discontinuation of nirmatrelvir-ritonavir or placebo
Results:
- 1296 patients randomized and included in full analysis population and 1288 received at least one dose of study interventions:
- Nirmatrelvir-ritonavir (n = 654) vs. Placebo Group (n = 634)
- Primary Outcome:
- Nirmatrelvir-ritonavir 12 days (95% CI: 11-13) vs Placebo 13 days (95% CI: 12-14)
- The primary outcome was NOT statistically significant, p=0.60
- Key Secondary Outcome:
- Overall: Nirmatrelvir-ritonavir 0.8% vs Placebo 1.6%; Difference from placebo (95% CI): -0.81 (-2.00-0.374)
- High Risk Group: Nirmatrelvir-ritonavir 0.9% vs Placebo 2.2%; Difference from placebo (95% CI): -1.29 (-3.26-0.67)
- Standard Risk Group: Nirmatrelvir-ritonavir 0.6% vs Placebo 1.0%; Difference from placebo (95% CI): -0.36 (-1.73-1.02)
- The difference was not significant
- Other Secondary Outcome:
- Overall COVID-19 related medical visits: Nirmatrelvir-ritonavir 2.3% vs Placebo 3.9%; least-squares mean ratio vs placebo: 0.50 (95% CI): (0.22-1.13)
- Overall mean number of days in the hospital per 100 participants: Nirmatrelvir-ritonavir 5 vs Placebo 18 (95% CI -0.22, -0.03)
- Viral load rebound: Nirmatrelvir-ritonavir 4.3% vs Placebo 4.1%
- Symptom rebound: Nirmatrelvir-ritonavir 11.4% vs Placebo 16.1%
- Adverse Events: Occurred in similar percentages of participants in the two groups and did not differ markedly between vaccinated and unvaccinated participants.
Strengths:
- The investigators asked a clinically relevant question with a primary outcome that focused on patient-centered outcomes.
- Adherence to protocol was noted to be 94.8% in the intervention group and 96.5% in the control group.
- Randomized double-blind controlled trial is the gold standard in scientific research and increases external validity of the findings.
- Investigators employed a large, international, multivendor study design with a diverse global enrollment that increases generalizability to a broader population.
Limitations:
- The cohort of vaccinated high-risk participants was enrolled regardless of the time since last vaccination.
- There were lots of exclusion criteria including patients with a previous history of COVID-19 infection or those who had received monoclonal antibodies, other antivirals, or convalescent plasma, likely introducing some selection bias.
- The median age was 42 and the patient population was 80% white. This relatively young and homogenous population limits generalizability to an older and more diverse cohort.
- Self-reporting of symptoms is very subjective and prone to bias.
- Blinding was likely affected as nirmatrelvir-ritonavir has a distinct taste, and in the setting of subjective self-reporting of symptoms, this can introduce significant information bias.
- Trial was done when the delta-variant was the dominant COVID-19 variant circulating in the population before the start of the Omicron wave. Therefore, the findings in this study may not be directly applicable to those individuals who are infected with lateral subvariants of SARS-CoV-2.
- The key secondary outcome is a composite endpoint. This is problematic as the purpose of composite outcomes is to drive down the size needed to show statistical significance and results are often driven by one component of the composite. In this study, hospitalizations drive the composite outcome primarily, whereas other secondary outcomes such as viral load are more disease-oriented.
- It is unclear how investigators arrived at the estimated 25% difference in time to sustained alleviation of all targeted COVID-19 signs and symptoms during their power calculation in their statistical analysis.
- The funders of this drug conducted this study and had a direct role in study design, data collection, data analysis, data interpretations, or writing of the report. This is a significant conflict of interest.
Discussion:
- Investigators attempt to shed light on a question with inconsistent consensus and practice patterns. Whether nirmatrelvir-ritonavir can confer a benefit in individuals who have been vaccinated or those without risk factors for severe disease in a time where we are seeing relatively milder cases of COVID in otherwise younger, healthier populations. In this trial, the investigators conclude that in their cohort of outpatient adults with COVID-19 who are at standard or high risk for severe COVID-19, there was no significant difference in time to symptom alleviation between the nirmatrelvir-ritonavir group and the placebo group.
- Despite being an industry-run trial that comes with significant sources of bias towards the intervention, this is a negative trial.
- It seems that as opposed to the EPIC-HR study, the benefit of nirmatrelvir-ritonavir does not seem to cross over to a population at lower risk for severe disease or to vaccinated individuals.
- The overall study population in this trial was a younger cohort of patients with a relatively low-risk population to begin with. The most common risk factors were BMI ≥ 30 kg in 17.8% of total patients, smoking (13.3%), followed by hypertension (12.3%) and diabetes (5.1%).
- This cohort of younger and relatively lower-risk populations is representative of patients who are seen in outpatient settings during the current climate of COVID-19.
- It may be that that if there was a larger percentage of vaccinated older, higher-risk conditions with more significant comorbidities, the results may have changed. This is difficult to tell, and further research would need to be done to see if there is any benefit in this subgroup of individuals treated.
- Regarding their key secondary outcome of COVID-19 related hospitalization or death from any cause through day 28, there are a few points to keep in mind.
- The authors do subtly allude to the nirmatrelvir-ritonavir vaccinated high-risk subgroup showing perhaps a signal towards benefit with less hospitalization, no deaths as well as no ICU admissions compared to the placebo group.
- It should be noted firstly that RCTs are powered for the primary outcome and not secondary outcomes. Any promising results from secondary outcomes should be strictly hypothesis generating and subject to future studies in additional RCTs.
- It should also be noted that the use of composite outcomes is problematic as one component of the composite can overwhelmingly drive the results, and that component may not be patient or disease-oriented.
- Additionally, composite outcomes serve to drive down the sample size needed to show statistical significance. The combination of this is likely to introduce publication bias, so, pooled estimates for these types of outcomes should be judged cautiously.
- Furthermore, this study is certainly underpowered for the composite analysis of COVID-19 hospitalization and death to even begin with.
- At the end of the day, the key secondary outcome needs to be interpreted within the above context.
- Future studies may certainly look at this question further, but there is not enough here to say that there is truly any signal to benefit of nirmatrelvir-ritonavir for these outcomes in the context of this trial.
- In this trial, it should be also noted that viral and symptom rebound were similar to the placebo group.
- An interesting note was that in the high-risk subgroup analysis, the nirmatrelvir-ritonavir group showed lower medical utilization/visits. This may be a focus of further research as the overall population in this study was relatively lower risk with fewer major comorbidities.
Author Conclusion: “The time to sustained alleviation of all signs and symptoms of COVID-19 did not differ significantly between participants who received nirmatrelvir–ritonavir and those who received placebo.”
Our Conclusion:
The study is large, and the results help to fill a gap in the literature on the use of nirmatrelvir-ritonavir in patients at lower risk for progression to severe COVID-19 as well as those who have been vaccinated. Based on the data, there is no high-quality evidence to support the use of nirmatrelvir-ritonavir in a low-risk population or in those who have been vaccinated. Further research is needed to address whether nirmatrelvir-ritonavir would be helpful in select cases such as patients with immunosuppressive diseases, active malignancy with treatment, etc or vaccinated high-risk individuals. In these cases, shared decision-making could be utilized to guide nirmatrelvir-ritonavir use.
Clinical Take Home Point:
Based on the current available evidence and landscape of COVID-19, routine use of nirmatrelvir-ritonavir is not recommended.
References:
- Hammond J, et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N Engl J Med. 2022. PMID 35172054
- Reis S, et al. Nirmatrelvir combined with ritonavir for preventing and treatment COVID-19. Cochrane Database of Syst Rev. 2023. PMID 38032024
- Hammond J, et al. Nirmatrelvir for Vaccinated or Unvaccinated Adult Outpatients with COVID-19. N Engl J Med. 2024. PMID 38598573
Guest Post By:

Carla Dugas, DO
Emergency Medicine Residency Program Director
Inspira Medical Center, Vineland NJ

Muhammad Durrani, DO
Associate Emergency Medicine Residency Program Director
Inspira Medical Center, Vineland NJ
Twitter/X: @ibbydurrani
Post Peer Reviewed By: Marco Propersi, DO (Twitter/X: @marco_propersi)

