
 Background: A series of tweets I sent out recently generated a visceral response from critical care clinicians the world over. I summarized my strategy of shock dose RSI as sedatives low and paralytics high (low dose ketamine, high dose rocuronium along with cardiovascular resuscitative strategies of push dose pressors and peripheral vasopressors). It seems that the visceral response and argument stems from EM’s desire to avoid peri-intubation arrest, and anesthesia’s equally strong desire to avoid awareness/suffering in the peri-intubation period. Typically ketamine is dosed at 1 – 2mg/kg IV followed by a paralytic agent prior to RSI. I have written a blog post on how to manage hypotension prior to RSI in shock patients HERE, but I wanted to write a separate post on this topic as it is difficult to carry on a meaningful conversation with the character limitations of twitter.
Background: A series of tweets I sent out recently generated a visceral response from critical care clinicians the world over. I summarized my strategy of shock dose RSI as sedatives low and paralytics high (low dose ketamine, high dose rocuronium along with cardiovascular resuscitative strategies of push dose pressors and peripheral vasopressors). It seems that the visceral response and argument stems from EM’s desire to avoid peri-intubation arrest, and anesthesia’s equally strong desire to avoid awareness/suffering in the peri-intubation period. Typically ketamine is dosed at 1 – 2mg/kg IV followed by a paralytic agent prior to RSI. I have written a blog post on how to manage hypotension prior to RSI in shock patients HERE, but I wanted to write a separate post on this topic as it is difficult to carry on a meaningful conversation with the character limitations of twitter.
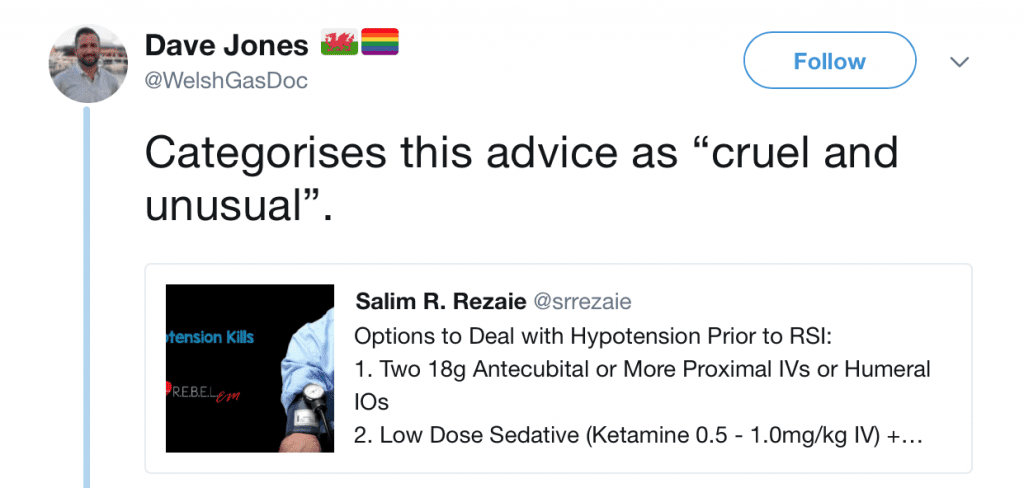
Here is my Original Tweet
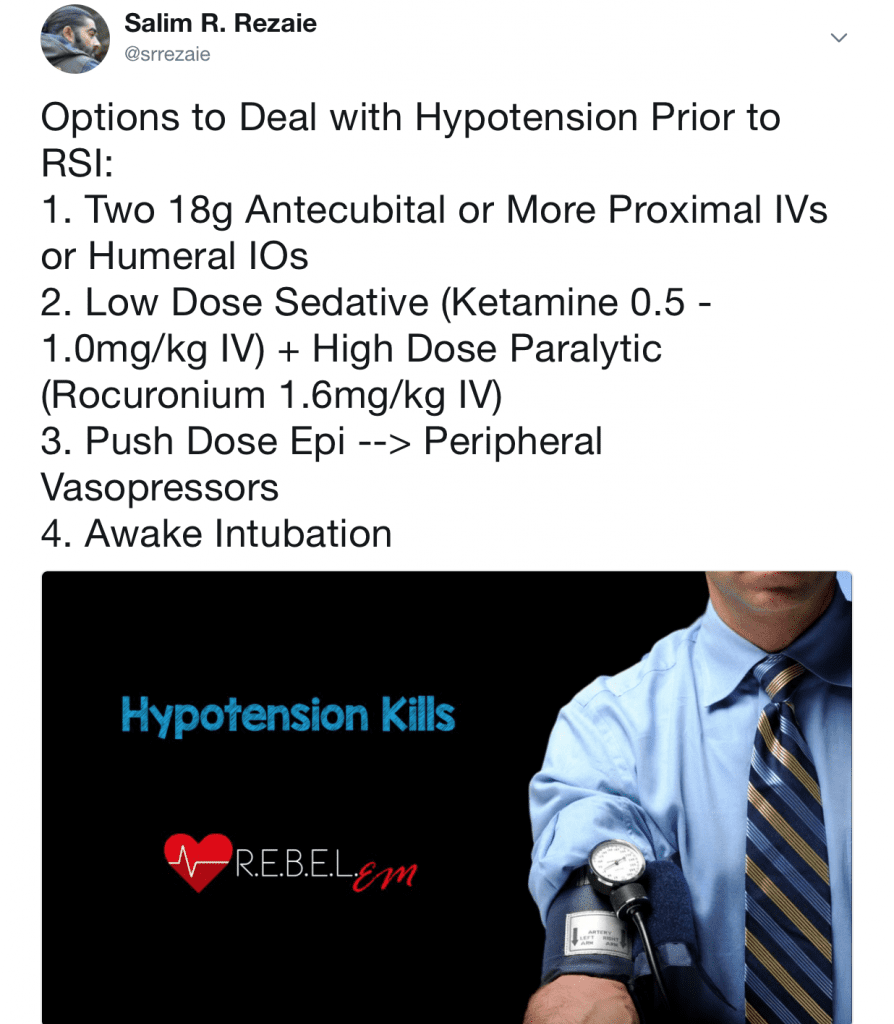
First to be clear, this is not a chronological order of things to be done, it is a potential list of options to prevent post intubation cardiac arrest. Second to be fair, many of the points brought up from this were correct but intubating a patient in shock is such a nuanced practice. Upon reflecting more on this topic I felt there were some very important points brought up in the engagement online and I wanted to be sure to cover all of them:
Resuscitate Before You Intubate
This is absolutely correct!!! In hypotensive patients requiring intubation, we should resuscitate before we intubate. 2 large bore IVs, IV crystalloids, and pressors. It is only after we have resuscitated these patients that we should then turn our attention to intubation, and not before (Important Caveat: There are some, very few cases, where immediate intubation is necessary prior to a full or even partial resuscitation).
Dosing of Ketamine for RSI in Shock Patients
There are several tweets, shown above, that have consternation with a lower dosing of ketamine for RSI. They are all right. No one should intubate a patient with just a low dose of an induction agent and then give them a paralytic as this is “cruel and unusual.” Being awake while being paralyzed is not an ok thing to do or have happen to a patient. On the other hand we don’t want to over-sedate either as this can lead to post intubation cardiac arrest, which itself is “cruel and unusual.”
Giving standard doses of ketamine (2mg/kg IV), can cause post-intubation hypotension in patients with shock. There was an observational trial of 112 patients with low blood pressure requiring intubation [1]. The authors calculated a shock index (Shock Index = HR/SBP) in all these patients prior to intubation. Patients found to have a high shock index (>0.9) not only didn’t have an increase in SBP (increase of 2mmHg), but 26% of them became hypotensive (1 in 4).
What I am advocating for is an individualized delayed sequence intubation (iDSI). Start at a lower dose of IV ketamine like 0.5mg/kg and then assess your patient. If they are not sedated, then give them another 0.5mg/kg. Continue to do this until you feel that your patient is completely sedated. Then and only then do you give paralytics. Remember shock in and of itself is a powerful anesthetic and these patients do not require full dose 2mg/kg IV ketamine and this practice can be deleterious. This should also be balanced with not under sedating our patients as, the idea of an awake paralysis is also rightfully horrifying.
More Evidence for Starting with Lower Doses of Ketamine in the Shock Patient Requiring RSI
- Heffner AC et al [2]: This was a retrospective cohort study of emergency intubations performed in a large, urban emergency department over a one year period. 542 patients underwent emergency intubation, and 410 met inclusion criteria. Cardiac arrest occurred in 17/410 (4.2%) of patients at a median of 6 minutes post intubation. This is 1 in 25 intubations. 2/3 of cardiac arrest occurred within 10 min of drug induction. Cardiac arrest was more common in patients experiencing pre-intubation hypotension (12% vs 3%; p < 0.002). Pulseless electrical activity was the initial rhythm in the majority of cases, but just over half of the cardiac arrests were successfully resuscitated. And no surprise here, but cardiac arrest was associated with increased odds of hospital death (OR 14.8; 95% CI 4.2 – 52).
- Kim WY et al [3]: This was a matched case control study with a primary outcome of arrest within 10 minutes of intubation.2,403 patients were included in this analysis and 41 patients (1.7%) had a post-intubation cardiac arrest within 10 minutes of the procedure. This is 1 in 60 intubations.The most common initial rhythm was pulseless electrical activity (78.1%). A systolic blood pressure of ≤90mmhg was independently associated with post-intubation cardiac arrest (OR 3.67; 95% CI 1.58 – 8.55).
- Dewhirst E et al [4]: This is a case report of two critically ill patients who experienced cardiac arrest following the administration of ≈2mg/kg of IV ketamine for rapid sequence intubation. The authors state, “The sympathomimetic effects of ketamine result in enhanced cardiovascular stability make it an extremely useful andesthetic agent. However, in patients with an exhausted endogenous catecholamine reserve, the unopposed direct negative inotropic effects of ketamine may lead to cardiovascular compromise.”
Dosing Paralytics High
Higher dose neuromuscular blocker is needed in shock due to circulation issues (We have to remember that these agents are cardiac output dependent medications). Succinylcholine possesses the fastest onset (45sec) and produces the shortest period of muscle relaxation (6 – 10min) compared to all other paralytic agents at standard doses. However, rocuronium dosed at 1.6mg/kg IV, gives the same onset of muscle relaxation as succinylcholine [6] and gives a longer safe apnea time [7] making it the preferred paralytic of choice in the critically ill patient. In critically ill patients in shock, use rocuronium 1.6mg/kg IV (Some advocate for 1.5mg/kg IV as this is easier to remember).
We are all Professionals
Just about everyone embracing the FOAM movement does so, because we are trying to improve patient care. A bunch of professionals, regardless of time zone, location of practice, or specialty coming together to engage with each other to become a better version of themselves and a better provider for our patients. We have many online conversations and some can become emotionally charged. However, the words we use and the way we use them can be harmful. There is no room for rudeness either online or at the workplace. There are studies that show this can be detrimental to patient care at the workplace [5] online engagement should be no different.
We are on the Same Team
 In the end we are all advocating for our patients. This is an important point to remember. Random tweets can be taken out of context and be misconstrued. amazing fake watches Just having a simple conversation whether it be online or in person can lead to many great things. The entire conversation about this topic was and still is just that, a conversation to improve patient care.
In the end we are all advocating for our patients. This is an important point to remember. Random tweets can be taken out of context and be misconstrued. amazing fake watches Just having a simple conversation whether it be online or in person can lead to many great things. The entire conversation about this topic was and still is just that, a conversation to improve patient care.
Twitter is NOT the End All Be All
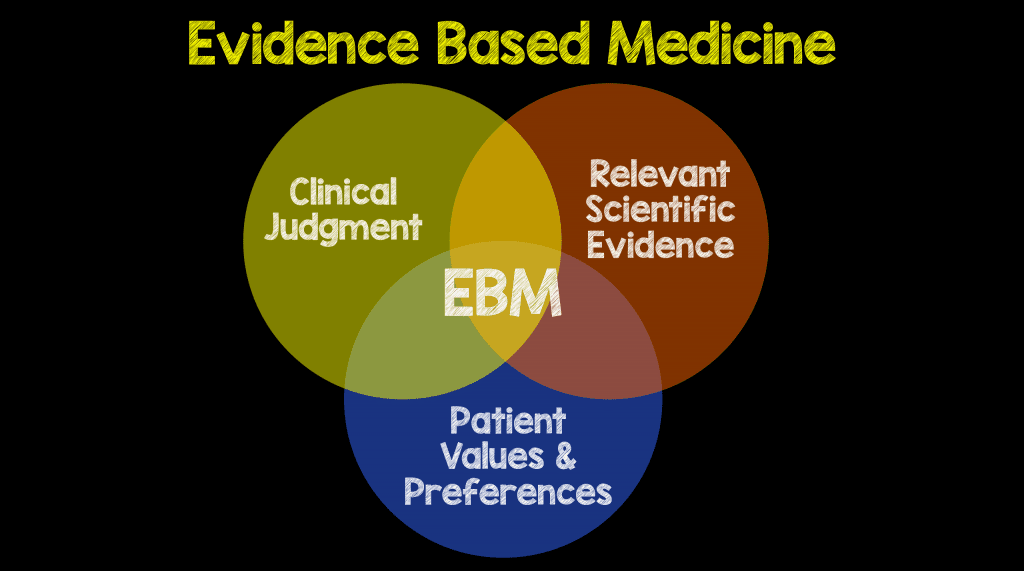
Anyone who has heard me speak knows I always say, don’t believe everything you read on the internet. You should always go and read the root literature, use your own critical thinking skills, and form your own opinions. Reading a blog post or listening to a podcast and just agreeing with the opinions of who wrote it blindly is the same as just reading an abstract without reading the entire paper. Both are equally dangerous practices. In the end blogs, podcasts, and social media are great to cut down knowledge translation and start a conversation, but it is up to each of us to review the primary literature to apply our own context. After all, evidence based medicine is not just about the root literature, but about provider experience, patient values/preferences, AND the relevant scientific evidence.
“The most important attribute that education can bring to anyone is the ability to think critically. In an era where information and knowledge is universally available, it is the power to comprehend, assess and analyze which makes the difference – those are the critical thinking skills.”
Charles Clarke, former UK Secretary of State for Education
References:
- Miller M et al. Hemodynamic Response After Rapid Sequence Induction With Ketamine in Out-of-Hospital Patients at Risk of Shock as Defined by the Shock Index. Ann Emerg Med 2016. PMID: 27130803
- Heffner AC et al. Incidence and Factors Associated with Cardiac Arrest Complicating Emergency Airway Management. Resuscitation 2013. PMID: 23911630
- Kim WY et al. Factors Associated with the Occurrence of Cariac Arrest After emergency Tracheal Intubation in the Emergency Department. PLoS One 2014. PMID: 25402500
- Dewhirst E et al. Cardiac Arrest Following Ketmaine Administration for Rapid Sequence Intubation. J Intensive Care Med 2013. PMID: 22644454
- Riskin A et al. Rudeness and Medical Team Performance. Pediatrics 2017. PMID: 28073958
- Curley GF et al. Rapid Sequence Induction with Rocuronium – A Challenge to the Gold Standard. Crit Care 2011. PMID: 22112346
- Taha SK et al. Effect of Suxamethonium vs Rocuronium on Onset of Oxygen Desaturation During Apnoea Following Rapid Sequence Induction. Anesthesia 2010. PMID: 20402874
For More Thoughts on This Topic Checkout:
- EMCrit Podcast 30 – Hemorrhagic Shock Resuscitation
- LITFL – Intubation, Hypotension, and Shock
Post Peer Reviewed By: Anand Swaminathan, MD (Twitter: @EMSwami) and Rob J. Bryant, MD (Twitter: @RobJBryant13)

