
 62 year old male with chief complaint of weakness. Patient had a complicated hospital course including necrotizing fasciitis which required surgical debridement and IV antibiotics. Patient was discharged home with oral antibiotics and returned to the ED with a chief complaint of weakness, abdominal pain, and 3 weeks of loose bowel movements.
62 year old male with chief complaint of weakness. Patient had a complicated hospital course including necrotizing fasciitis which required surgical debridement and IV antibiotics. Patient was discharged home with oral antibiotics and returned to the ED with a chief complaint of weakness, abdominal pain, and 3 weeks of loose bowel movements.
BP: 100/51 HR 93 RR 16 Temp 97.2 O2 Sat 98% on RA
ECG from triage is shown…
Before reading on, try to come up with your own interpretation of this ECG before moving on to the final impression
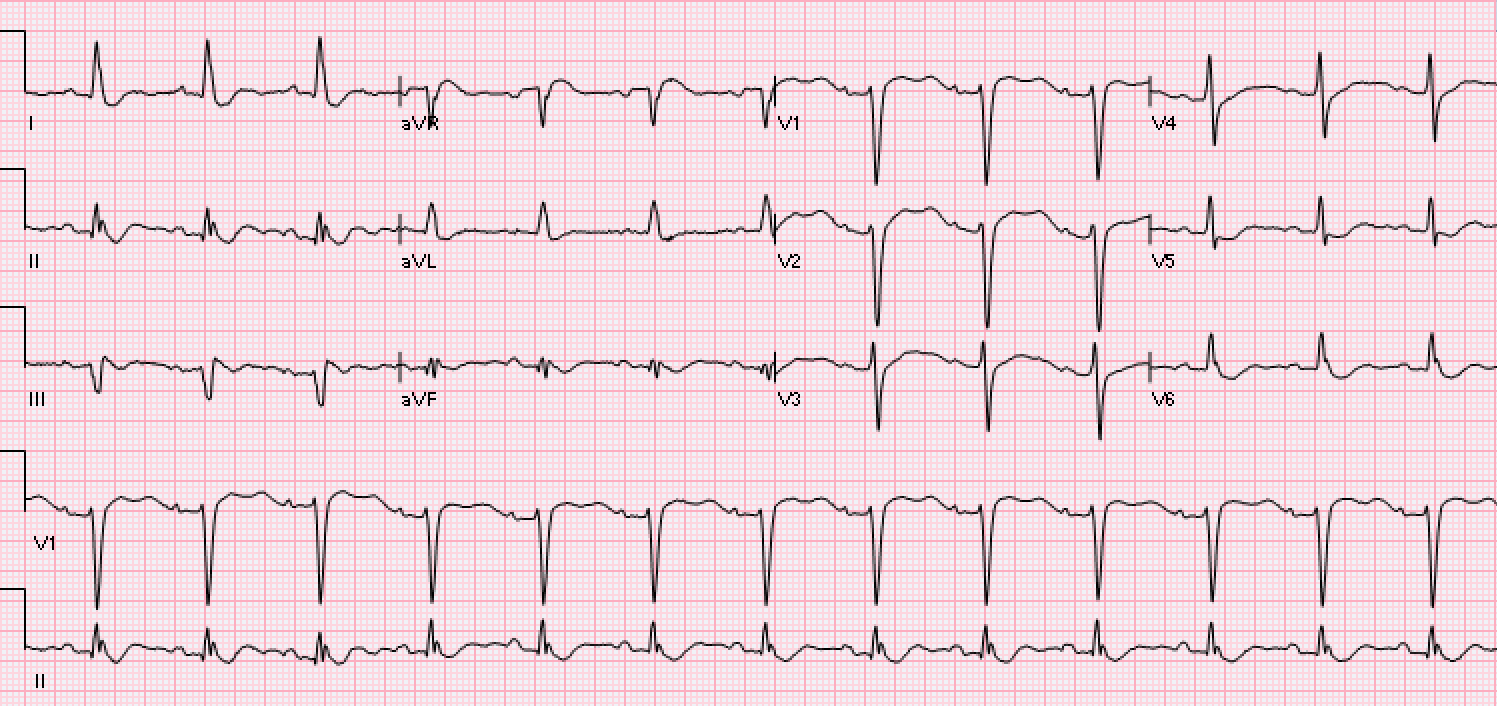
- Rate: Ventricular rate 81
- Rhythm: Normal Sinus Rhythm
- Axis: Normal Axis
- Final ECG Interpretation: U waves consistent with hypokalemia
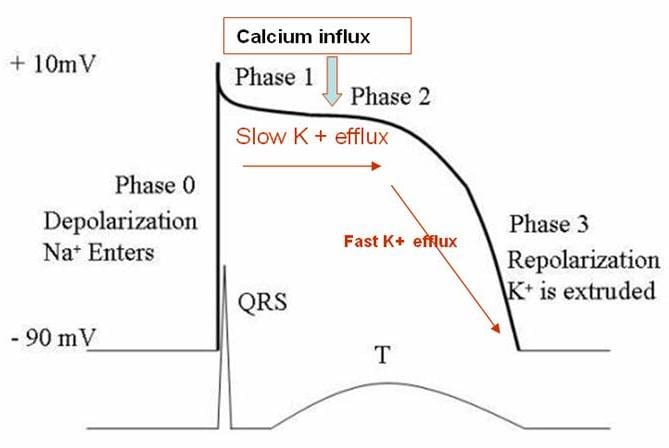
Hypokalemia is the most common electrolyte abnormality encountered in clinical practice (i.e. K+ <3.6 mmol/L seen in over 20% of hospitalized patients) [1]. As serum potassium levels decline, the transmembrane potassium gradient is decreased causing an elevation in the resting membrane potential and a prolongation of the action potential (Phase 3 repolarization). Therefore, the earliest ECG changes associated with hypokalemia is decreased T wave amplitude [2]. At extreme, low levels of potassium a positive deflection after the T wave (U wave) can be seen. The U wave is best seen in the mid-precordial leads (i.e. V2 and V3) [2].
What are some electrocardiographic findings associated with hypokalemia? [2]
- Flattening of T wave
- T wave inversion
- ST segment depression
- Prominent U waves
- Prolongation of QT (U) Interval
- Ventricular tachycardia
- Torsades de pointes
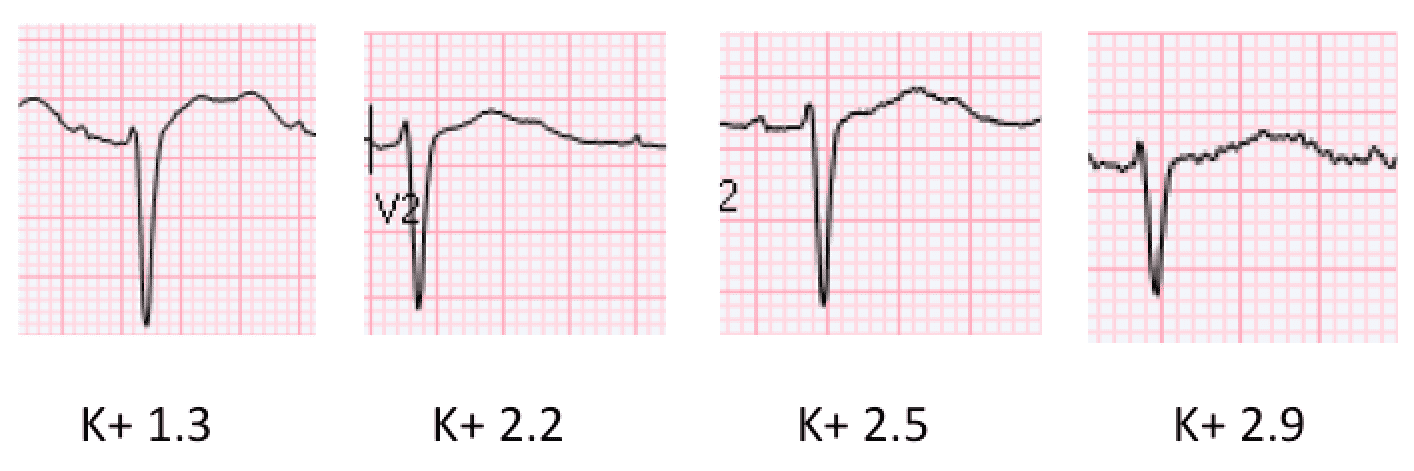
Case Conclusion: Patient was diagnosed with C. Diff Colitis. Initial K+ was 1.3 shown on the ECG above. Potassium was aggressively replaced and ECG changes in lead V2 are shown as the potassium started to correct below.
References:
- El-Sherif N et al. Electrolyte Disorders and Arrhythmogenesis. Cardiol J 2011. PMID: 21660912
- Diercks DB et al. Electrocardiographic Manifestations: Electrolyte Abnormalities. JEM 2004. PMID: 15261358

