

What They Did:
- Single center, prospective, randomized, double-blind clinical trial
- 240 patients, 18 – 65 years of age with renal colic
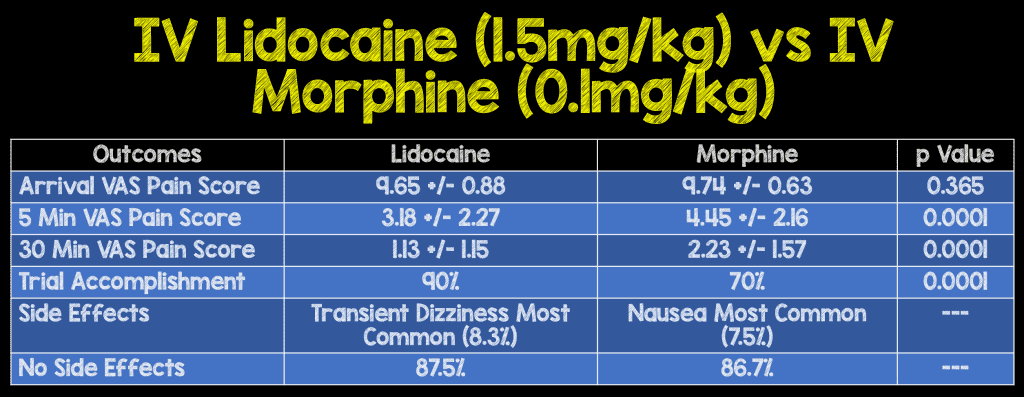
- comparison of IV preservative free 2% lidocaine (1.5mg/kg) vs IV morphine (0.1mg/kg)
Outcomes:
- Visual Analogue Pain Scale (VAS) of 0 – 10 at time of arrival, 5, 10, 15, and 30 minutes after injection
- “Trial Accomplishment” = VAS pain score of <3 for 30 minute after the last analgesic dose or the entire 10mL of solution in the syringe was used up.
Inclusion:
- Patients aged 18 – 65 years
- Unilateral abdominal pain and positive hematuria on urinalysis
Exclusion:
- History of renal, hepatic, or cardiac (ischemic heart) disease
- Allergy to lidocaine or morphine
- Inability or unwillingness to give written informed consent
- Pregnancy
Results:
Strengths:
- Double-blind, randomized clinical trial
- Injection of medications and filling out questionnaires performed by another person not involved in the research project
- Similar looking 10mL syringes were used for either 10mg of morphine or 200mg of lidocaine
Limitations:
- Single center study
- Non-steroidal anti-inflammatory drugs (NSAIDs) shown to relieve colic pain, not discussed in this paper.
- Patients with history of renal disease, liver disease and heart disease were excluded
- Primary endpoint of this study is not clear. Was it pain change at 5, 10, 15, or 30 minutes?
- “Trial accomplishment” was considered to have been achieved when: VAS pain score of <3 for 30 minute after last analgesic dose OR the entire 10mL of solution in the syringe was used up. There is no discussion of how many patients achieved pain <3 and how many used up the entire 10mL syringe.
- Kidney stone diagnosis confirmation was made by use of Kidney, Ureter, and Bladder (KUB) radiographs and ultrasound studies, neither of which are the gold standard in diagnosis of nephrolithiasis
Discussion:
- All enrolled patients received IV metoclopramide (0.15mg/kg)
- Lidocaine toxicity generally doesn’t start occurring until higher doses of 4 – 6mg/kg, which include lightheadedness, perioral numbness, dizziness, and transient hypertension. Cardiac toxicity occurs at even higher doses than this.
- Both lidocaine and morphine seem to decrease pain, but the clinical significance of one medication over the other is not clear
- There has been a 2nd double-blind, RCT published [2] in 2016 that randomized 110 patients, aged 18 – 50 years of age. Patients received IV morphine 0.1mg/kg + IV lidocaine 1.5mg/kg or IV morphine 0.1mg/kg + Normal Saline Placebo. Pain and nausea were rated on a 10 point VAS. There was no statistical difference in persistence of pain between the groups, however the lidocaine group had significantly less time feeling nauseated: 58.33 min vs 26.6 min. The clinical significance of this is unclear as there plenty of alternatives to nausea.
- Addendum 06/13/2018: Since the publication of this blog post I have been asked how to infuse IV lidocaine and here is how I run it: 2% preservative free (cardiac) IV lidocaine 1.5mg/kg (max dose 200mg) mixed in a 100mL saline bag run over 10minutes.
Author Conclusion: “Changing the smooth muscle tone and reducing the transmission of afferent sensory pathways, lidocaine causes a significant reduction in pain.”
Clinical Take Home Point: IV preservative free (cardiac) lidocaine (1.5mg/kg) seems to be another opioid sparing treatment option in our armamentarium to treat renal colic pain in patients without renal, liver, or cardiac disease, however this single study should not change practice of using NSAIDs as first line opioid sparing therapy where available.
References:
- Soleimanpour H et al. Effectiveness of Intravenous Lidocaine Versus Intravenous Morphine for Patients with Renal Colic in the Emergency Department. BMC Urology 2012; 12(13): 1 – 5. PMCID: PMC3508963
- Firouzian A et al. Does Lidocaine as an Adjuvant to Morphine Improve Pain Relief in Patients Presenting to the ED with Acute Renal Colic? A Double-Blind, Randomized Controlled Trial. Am J Emerg Med 2016; 34(3): 443 – 8. PMID: 26704774
For More on This Topic Checkout:
- Ken Milne at The SGEM: SGEM #202 – Lidocaine for Renal Colic?
- ALiEM: Intravenous Lidocaine for Renal Colic
Post Peer Reviewed By: Anand Swaminathan (Twitter: @EMSwami)

